


a. What are uterine fibroids? Are they early signs of uterine cancer?
Uterine fibroids are noncancerous growths of the uterus that often occur during a woman’s childbearing years. They are also called fibromyomas, leiomyomas or myomas and are not associated with an increased risk of uterine cancer and only 1% ever become cancerous. Uterine fibroids develop from the smooth muscular tissue of the uterus (myometrium). A single cell reproduces repeatedly, eventually creating a pale, firm, rubbery mass distinct from neighboring tissue.
b. Are fibroids age related? Who are prone to having fibroids?
Yes, as they tend to be found in women of childbearing age. A strong family history (mother, sister with fibroids) increases one risk of developing fibroids as is race. Afro-Caribbean women have a higher risk and fibroids tend to occur at a younger age, develop more and are larger in this group of women.
c. What are the symptoms of fibroids?
3 out of 4 women have uterine fibroids sometime during their lives, but most are unaware of their existence because they are often asymptomatic. They may be discovered incidentally during a pelvic exam or pelvic ultrasound scan. If symptoms occur, the most common symptoms of uterine fibroids include:
- Heavy menstrual bleeding (menorrhagia)
- Prolonged menstrual periods (lasting 7 or more days)
- Pelvic pressure or pain
- Frequent urination (frequency)
- Difficulty emptying your bladder (urinary retention)
- Constipation
- Backache
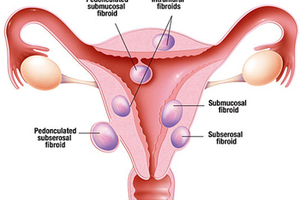
Very rarely, a fibroid can outgrow its blood supply and begin to die causing acute pain. A fibroid that hangs by a stalk inside or outside the uterus (pedunculated fibroid) can twist on its stalk and cut off its blood supply leading to acute pain. Symptoms and signs are related to the location of the fibroid.
- Subserosal fibroids project to the outside of the uterus and sometimes press onto the bladder, causing urinary symptoms. If fibroids bulge from the back of the uterus, they occasionally can press either on the rectum, causing constipation, or on the spinal nerves, causing backache.
- Submucosal fibroids grow into the inner cavity of the uterus and are thought to be the main cause for prolonged, heavy menstrual bleeding and can be a problem for women attempting pregnancy (miscarriage).
d. What kinds of investigation are available to determine if one has fibroids?
Fibroids are commonly diagnosed on pelvic ultrasound scans. Computerized tomography (CT) and magnetic resonance imaging (MRI) can also be employed but are more costly. Hysterosonography uses sterile saline to expand the uterine cavity, making it easier to obtain interior images of the uterus with an ultrasound scan. This test may be employed if there is heavy menstrual bleeding despite normal results from traditional ultrasound. Hysterosalpingography uses a dye to highlight the uterine cavity and fallopian tubes on X-ray images. In addition to revealing fibroids, it can determine fallopian tube patency at the same time for women experiencing concurrent infertility. Hysteroscopy involves inserting a small, lighted telescope through the cervix into the uterus simultaneously distending the uterine cavity with saline thereby facilitating direct examination of the uterine cavity.
e. How are fibroids removed or treated? Will they affect a patient’s fertility if nothing is done or after treatment?
For the majority of women who are asymptomatic, routine follow up ultrasound scans to detect for any increase in size or number is recommended as they are not cancerous, grow slowly and tend to shrink after menopause when levels of female hormones drop. Medications for uterine fibroids act on hormones that regulate menstrual cycle and treat the symptoms (heavy menstrual bleeding, pelvic pressure). They do not remove fibroids, but may shrink them. Medications include:
- Nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives or progestins control menstrual bleeding, but do not reduce fibroid size.
- Progestin-releasing intrauterine system (IUS) like Mirena can relieve heavy bleeding and pain caused by the fibroids provided the fibroids do not distort the uterine cavity. IUS does not shrink fibroids or make them disappear.
- Gonadotropin-releasing hormone (Gn-RH) agonists decrease oestrogen and progesterone levels, thereby stopping menses and shrinking fibroids.
- Danazol (synthetic drug similar to testosterone) may stop menstruation, correct anemia and even shrink fibroid tumours and reduce uterine size. Occasional side effects, such as weight gain, dysphoria (feeling depressed, anxious or uneasy), acne, headaches, unwanted hair growth and a deeper voice, make this drug an unpopular choice.
Surgical treatment is recommended when fibroids are too big, too numerous, rapidly growing (potentially malignant) and when medical treatment fails.
Myomectomy involves removeing the fibroids but leaving the uterus behind. This is the treatment choice if fertility is desired. There is a risk of fibroid recurrence. There are 3 types of myomectomy:
- Abdominal myomectomy (open method) is preferred if there are multiple fibroids, very large or very deep fibroids.
- Laparoscopic myomectomy (minimally invasive surgery) uses slender instruments inserted through small incisions in the abdomen to remove the fibroids. Small and large fibroids can be removed this way depending on the skill of the gynaecologist. The main advantage over the abdominal method is that it is associated with a faster recovery time, less discomfort, shorter hospital stay and cosmetically more pleasant.
- Hysteroscopic myomectomy may be preferred if the fibroids are contained inside the uterus (submucosal). A long, slender scope (hysteroscope) is passed through the vagina and cervix into the uterus. The fibroid is then resected out under direct visualization with the hysteroscope.
Hysterectomy (removal of the uterus) is the only permanent solution for uterine fibroids but patients will not be able to conceive after this. It can be performed abdominally (open method), laparoscopically (minimally invasive surgery) or vaginally.
There are other procedures to shrink or destroy fibroids without actually removing them through surgery.
- Endometrial ablation is performed with a special instrument inserted into the uterus using heat to destroy the lining of the uterus therefore stopping menstruation or reducing menstrual flow. It is effective in stopping abnormal bleeding, but does not affect fibroids outside the inner lining of the uterus.
- Uterine artery embolization involves injecting small embolic agents into the arteries supplying the uterus cutting off blood supply to the fibroids. The fibroids then shrink. Advantages over surgery include no incision and a shorter recovery time but complications may occur if the blood supply to the ovaries or other organs is compromised.
f. Can medication alone be effective in getting rid of fibroids? Why or why not?
See above. Medical treatment can fail if the fibroids are too big, too numerous or rapidly growing (potentially malignant).
Dr Christopher Ng
GynaeMD Women's & Rejuvenation Clinic
#04-03A Camden Medical Centre
1 Orchard Boulevard
Singapore 248649
Tel: 67338810
Email: gynaemd@singnet.com.sg
Website: www.gynaemd.com.sg




